

(To find data for yourself go to pubmed and put in the words "Computed Tomography radiation dose")
Here is a 2012 ISRN Gastroenterology article discussing stomach catscans in Inflammatory Bowel Disease. (pdf)
Here is a 2007 New England Medical Journal article.(pdf)Read this 2007 article thoroughly.
The 2007 article shows are that whereas in 1980, there were about 3 million catscans yearly, by 2005, there were around 62 million yearly (72 million were performed by 2007). The authors suggested that around one third of catscans are unnecessary and could have been replaced with non-radiation technology, which means that around 20 million catscans subjected patients to unnecessary risk..
Every cat scan has an adult radiation dose of around 10 mSv, and paediatric dose of 20 mSv. Usually, two to three scans are performed, but sometimes even more. CT (computed tomography) scans cause around 2 per cent of all cancers primarily lung and colon. About 11 per cent of all CT scans were carried out on children to determine if they have appendicitis, and researchers considered that children were at greater risk of developing cancer because their radiation load continues to increase as time goes on.
The study estimated that around 2% of cancers could be caused by catscans, and discusses doses, comparing catscans with survivors from Nagasaki and Hiroshima who received doses of between 5 - 150 mSv.
The study also felt that part of the problem was that doctors didn't feel that catscans emitted more radiation than ordinary xrays.Another 2007 study showed that most doctors underestimate radiation amounts.
Quote:
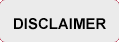
In summary, there is direct evidence from epidemiologic studies that the organ doses corresponding to a common CT study (two or three scans, resulting in a dose in the range of 30 to 90 mSv) result in an increased risk of cancer. The evidence is reasonably convincing for adults and very convincing for children.
Here is the dose chart from the NEMJ 2007 article:
In reality though these doses cannot be trusted because a study in 2009 found the following:
"We documented higher and more variable doses than what is typically quoted from the most common types of diagnostic CT studies performed in clinical practice. For example, the median effective dose of an abdomen and pelvis CT scan (the most common type of CT examination performed in the United States) is often quoted as 8 to 10 mSv. Yet we found that the median dose of a routine abdomen and pelvis CT scan was 66% higher, and the median dose of a multiphase abdomen and pelvis CT scan was nearly 4-fold higher.”
Hence the 2012 warning by FDA.
However, the risks as stated in the 2003 ABC programme are still relevant, even though doses have supposedly been reduced since then... because those children who had those scans in 2003 are now adolescents. Since the ABC programme on catscans is no longer in the archives, I'm going to put the transcript up here in full. And since there has been much discussion on the radio about going to Mars, the 2003 programme has interest there as well.
Environmental Radiation 25 August 2003
Professor Eric Hall from Columbia University in New York has extensively studied the impact of environmental radiation. He's attended the International Congress of Radiation Research in Brisbane where he presented his findings.
Norman Swan: Welcome to the program.
This week on The Health Report, putting care in the hands of the person who’s got the problem; does it work, and how does it compare to seeing the quack regularly?
The role of death in treating asthma;
And comparing the impact of Hiroshima and Nagasaki to everyday X-rays and the risk of space travel.
Professor Eric Hall from Columbia University in New York has spent much of his career studying the impact of environmental radiation. He’s been here in Australia presenting his findings to a conference in Queensland.
Eric Hall: The interest in environmental radiation is to look at the levels to which human beings are exposed from natural background radiation, radiation that comes in out of space, radiation that comes out of the ground, radiation that we have in our food, and contrast this to the sort of radiation levels that astronauts are exposed to when they’re in the shuttle and much more so if a visit to Mars comes off where the radiation levels would be very much higher. NASA is one of the major funders of radiation research in the United States now.
Norman Swan: So when you do those calculations, before we get to the medical applications, when you do those sorts of calculations, and maybe even extrapolate it back to what most people go back to, Hiroshima and Nagasaki where you had populations in the sphere of exposure to known radiation, what sort of story evolves in terms of our regular everyday exposure versus space travel, versus what we know from Japanese populations?
Eric Hall: Well the study of the exposed Japanese survivors of the A-bomb attacks is certainly the gold standard, because a huge amount of money was spent on it over a period of more than 50 years, and no other comparable study has ever been done, or is likely to be done. So that’s why we keep going back to that. In fact as we often say, people think of that as a high dose study, but in fact most of the people that are now alive 50, 60 years after Hiroshima and Nagasaki, it was quite a low-dose study.
Norman Swan: The high dose people have died?
Eric Hall: No, most of them didn’t die from radiation, they died from blast and heat within the first half kilometre. But anyway, the doses are higher than we get from natural background by two orders of magnitude nevertheless, but they are not higher than astronauts will get on a trip to Mars.
Norman Swan: Really?
Eric Hall: They’re comparable. And not only that, but the other thing that’s quite interesting is that the doses of radiation that one gets in diagnostic radiology in terms of the helical CT scan overlaps with the bottom end of the doses to which the Japanese were exposed and which show an elevation in solid cancer incidence now, 50 years later.
Norman Swan: So you’re saying one helical CT scan corresponds to an X-ray dosage similar to peripheral survivors of Hiroshima and Nagasaki?
Eric Hall: Oh yes. In the study we did, which is probably one of the most useful things I’ve ever done in terms of achieving any result, is we published a paper which calculated the risks involved in a helical CT scan of the abdomen in children. They’re very common in the United States.
Norman Swan: And we should just say a helical CT is the modern form of CAT scanning which is much more rapid, where you get a kind of spiral picture where it can be done in a matter of moments, rather than a slow process of repeated slices.
Eric Hall: This is particularly useful and important in children, because it’s fast, and therefore you don’t need to sedate the child. And so if you do a helical or spiral CT scan of the abdomen of a one-year-old child, it’s almost total body irradiation and the dose involved to all the internal organs is of the order of 5-15 rads, and the Japanese data go down to about 5-rads.
Norman Swan: Rad being a measure of radiation exposure.
Eric Hall: Rad being a measure of radiation exposure. So you are able to use these data from the Japanese to make an estimate of the risk from a helical CT scan without using any assumptions about the shape of a model or an extrapolation below the dose range for which data are available, that’s the important point.
Norman Swan: And are we talking here about total body exposure, or exposure to bits of the body? Because this does go to the issue of both space travel and medical treatments. When we have radiotherapy it tends to be pretty confined.
Eric Hall: Well when it comes to the induction of cancer by radiation, all of the evidence we have, for example, for the risk of breast cancer, the incidence of the function of dose is much the same.
Norman Swan: Which is why some people who’ve had Hodgkin’s Disease as teenagers, women, who’ve had radiotherapy to the chest area, are at high risk of breast cancer about 18 to 20 years later?
Eric Hall: That’s right. Forty times higher or something like that, very high.
Norman Swan: So just give us a picture, let’s go back to this helical CT, and the Hiroshima survivors, just compare what 50 years later the Hiroshima and Nagasaki survivors are getting for the equivalent dose of radiation.
Eric Hall: You mean in terms of cancer incidence?
Norman Swan: Yes.
Eric Hall: The increased incidence is very small. If you look at the 100,000 people that have been studied very carefully for 50-odd years, something like 12,000 of those have died of cancer naturally over the years.
Norman Swan: So that’s the expected number.
Eric Hall: That’s the expected number, and the number from the control group, and about 500 excess cancers involving all dose groups. It’s about 500 extra, (Hilary - I don't consider an "excess" of 500 cancer cases from 100,000 people to be small, particularly when universal vaccination is "justified" on complication rates from disease being much smaller than that.) so it’s not a very big increase considering the whole population was exposed to a nuclear weapon.
Norman Swan: Take me on that line to the use of regular radiology, you know X-ray imaging.
Eric Hall: We calculated that a one-year-old child having an abdominal helical scan had about a one in a thousand chance of developing cancer, (Let's just repeat that shall we? Giving a one year old a cat scan results in a 1 per 1,000 chance of cancer as a result) and since there are 2.6-million children scanned every year in the United States, that would suggest that you are quite possibly producing a public health problem for the future.
Norman Swan: What about adults getting helical CTs?
Eric Hall: Well adults are bigger than one-year-old children, so that the proportion of their total body irradiated for a given sized scan is much less, and secondly, a mature adult say 50, 60 years old, is about 15 times less sensitive to radiation-induced cancer than a one-year-old child.
Norman Swan: So for adults, it’s less of an issue ?
Eric Hall: I would say for any situation where the medical problem urgently needs a CT scan, it shouldn’t be an issue, but it argues against using helical CT scans in sort of a screening mode, which in many ways they are used in the United States.
Norman Swan: So in other words, these people who are going for a whole body scan which has been a very popular marketing ploy here, although recently banned in at least one State, is not a sensible thing to have done, because you might as well have stood on the edge of Nagasaki in 1945.
Eric Hall: Not a very sensible idea I would say.
Norman Swan: What about space travel? Does this make it impractical to do a manned trip to Mars?
Eric Hall: It’s borderline. Whether humans beings can have the journey to Mars, spend some time on Mars, and come back without getting a dose of radiation that is lethal, is marginal at the moment.
Norman Swan: Lethal? So it’s that much?
Eric Hall: Yes.
Norman Swan: So it’s equivalent to the high dose in a nuclear bomb going off?
Eric Hall: Yes. NASA is spending a lot of money trying to look for protectors and of course trying to devise ways to shield and protect astronauts, but at the moment it’s being talked about, but whether it will ever happen I’m not sure.
Norman Swan: What about radiotherapy? How does this apply to radiotherapy, which it’s argued, at least in the Australian context, is actually under-used in people with cancer, and probably about 20% or 30% more people need to have radiotherapy according to the evidence, than are having it at the moment; what are the risks there?
Eric Hall: Well in most instances it’s very difficult to get an assessment of the possible induction of malignancy in cancer patients because you don’t have a good appropriate control group. Now the two big exceptions for that are carcinoma of the cervix in women and prostate cancer in men. In particular we’ve taken a very careful look at prostate cancer and there you do have a good control group because –
Norman Swan: Some may choose not to be treated.
Eric Hall: Some may choose to have surgery. So we came up with 50,000 patients treated with radiotherapy, and 70,000 patients that had a prostotectomy –
Norman Swan: With no radiotherapy.
Eric Hall: No radiotherapy, and where they were matched for other factors. And to cut a long story short, we found that there was about a 1 in 70 chance of developing a radiation-induced second malignancy after about ten years. The incidence goes up with time, after radiation, by five years it’s barely detectable, but by ten years it’s about 1 in 70, and involves the bladder, it involves part of the GI tract, and even as far away as the lung, you get a very small increase in second malignancies. ( Hilary Do you call 1 in 70 small?) So again, in instances where radiotherapy is the best way to treat, it’s a small downside to an otherwise very effective treatment.
Norman Swan: But it’s important so that you can make an informed decision?
Eric Hall: That’s right, and the other part is we’ve taken a look at the new developments that are potentially very exciting, the use of IMRT, or Intensity Modulated Radio Therapy. The idea here is to concentrate the radiation dose more accurately in the tumour and reduce the high dose to the normal tissue surrounding the tumour, and the idea is that this should improve cure rates.
Norman Swan: It’s almost like applying a magnifying glass to the sun, it’s really getting it highly focused on a tiny bit of tissue.
Eric Hall: That’s a very good analogy, yes indeed. The downside from our point of view is that in order to do this procedure it means that a much bigger volume of normal tissue is treated. Instead of using typically four beams coming in from four directions, you may use eight, nine or ten beams.
Norman Swan: These are like the entry tracks for the beams before they concentrate on the hot spot in the middle?
Eric Hall: That’s right. So you end up irradiating a much bigger volume of normal tissue in these techniques.
Norman Swan: But with a lower dose?
Eric Hall: But with a lower dose. And there is good reason to believe that that significantly increases the risk of an induced malignancy in those normal tissues.
Norman Swan: So what do we do with all this information? Well first of all, I’m not going to Mars, you’ve convinced me. I’ll hand back my ticket, that’s the first thing you’ve done. And I’ll certainly not have a whole body scan with helical CT. But with radiotherapy?
Eric Hall: Well again, we’re talking about going to these new techniques, and I think it’s important that the people that advocate going to these new techniques have got to prove that the benefit of the new techniques outweighs any potential downside. I think it’s important that we have all of the information available before big decisions are taken.
Norman Swan: Eric Hall is Professor of Radiation Biophysics and Director of the Center for Radiological Research at Columbia University in New York.
References:
Hall EJ, Wuu CS Radiation-induced second cancers: the impact of 3D-CRT and IMRT. Int J Radiat Oncol Biol Phys.2003 May 1;56(1):83-8
Hall EJ Lessons we have learned from our children: cancer risks from diagnostic radiology. Pediatr Radiol. 2002 Oct;32(10):700-6. Epub 2002 Jul 19
Hall EJ. Helical CT and cancer risk. Pediatr Radiol. 2002 Apr;32(4):225-7. Epub 2002 Mar 06
Hall EJ. Invited editorials: CT scanning; risk versus benefit. J Radiol Prot.2000 Dec;20(4):347-8
The following URLS may also not work. They were collected 8 years ago
http://www.ki4u.com/Secret_Fallout/SFchp3.html
Yet, as I well knew from my own research, the reason why so much effort was being spent to reduce the dose from medical X-rays was that the doses of only a few rads per year received by radiologists in the course of their work had been found to decrease their life spans significantly, while among their children there had been a definite increase in congenital defects. Furthermore, if Dr. Stewart was correct, only 1 to 2 rads would double the chances of a child developing cancer when the radiation was received in the last few months of the mother's pregnancy, and only one-tenth of this amount might have the same effect when received in the first few months.
200 to 400 millirads was roughly equivalent to the dose from a pelvic X-ray
http://www.ki4u.com/Secret_Fallout/SFchp6.html
Late in 1966, I was given a copy of the preliminary results of a Yale University study of Hiroshima and Nagasaki carried out by Dr. S. Finch and a group of colleagues and sponsored by the Atomic Bomb Casualty Commission. The study involved an examination of the incidence of leukemia among some 17,000 children whose parents had been within 2000 meters of the explosions. Radiation doses ranged from about 3 to 30 rads, with a few as large as a hundred. These were certainly much larger than the doses from typical pelvic X-rays received by the mothers in the study by Dr. Saxon Graham, doses which increased the risk of childhood leukemia among the children conceived many years later by as much as 100 percent.
In the case of Nagasaki, the fallout had been even heavier, giving external doses as high as 100 rads in the suburb of Nishiyama.
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?holding=npg&cmd=Retrieve&db=PubMed&list_uids=286106&dopt=Abstract
J Natl Cancer Inst. 1979 Jun;62(6):1347-59.
Malignant breast tumors among atomic bomb survivors, Hiroshima and Nagasaki, 1950-74.
Tokunaga M, Norman JE Jr, Asano M, Tokuoka S, Ezaki H, Nishimori I, Tsuji Y.
For 1950-74, 360 cases of malignant breast tumors were identified among the 63,000 females of the Radiation Effects Research Foundation's (Hiroshima and Nagasaki) Extended Life-Span Study sample of survivors of the 1945 atomic bombings of Hiroshima and Nagasaki; 288 of these females were residing in one of these two cities at the time of bombing (ATB). Two-thirds of all cases were classified as breast cancers on the basis of microscopic review of slides, and 108 cases received an estimated breast tissue dose of at least 10 rads. The number of cases of radiogenic breast cancer could be well estimated by a linear function of radiation dose for tissue doses below 200 rads. Excess risk estimates, based on this function, for women 10-19, 20-29, 30-39, and 50 years old or older ATB were 7.3, 4.2, 2.6, and 4.7 cases per million women per year per rad, respectively. Women irradiated in their forties showed no dose effect. Among all women who received at least 10 rads, those irradiated before age 20 years will have experienced the highest rates of breast cancer throughout their lifetimes. Separate excess risk estimates for Hiroshima and Nagasaki did not differ significantly, which indicates that for radiogenic breast cancer the effects of neutrons (emitted only in the Hiroshima explosion) and gamma radiation were about equal. Radiation did not reduce the latency period for the development of breast cancer, which was at least 10 years. The distribution of histologic types of cancers did not vary significantly with radiation dose. The data suggested that irradiation prior to menarche conferred a greater risk than irradiation after menarche.
PMID: 286106 [PubMed - indexed for MEDLINE]
http://www.xenophilia.com/str_rad.htm
The rad represents a certain dose of energy absorbed by 1 gram of tissue. (For most purposes, 1 rad = 1 rem = 0.01 sievert = 0.01 gray). Okay, how many rads have you had? This is avoidable radiation ( values in mrads. )
595 to 710 mrads - - Upper GI Series
.5 to 400 mrads - - Dental Bite-Wing
78 to 330 mrads - - Skull
44 to 143 mrads - - - Chest
NOTE: The dose of radiation needed for one chest x-ray has dropped from 20 rads in the 1920's to under 0.2 rads in 1995 - 1
Typical chest x-ray exposure: 10 - 100 mrads. Exposure of 50 rads causes radiation sickness. Dosages exceeding 200 rads can cause death. - 2
Since 1 mrad = 0.001 rad then it takes 1000 mrads to take 2.69 days off of your life (this is not a confirmed fact, it is just an estimate based on our guess from above). For every dental bite-wing x-ray (400 mrad) , subtract one day plus one hour and 49 minutes from your life. Said another way, a day is subtracted for every 371.7 mrads. A single dental bite-wing x-ray gives you over a YEARS WORTH of radiation damage.