

On November 16th, 2010, Vaccine published an article titled “Public vaccination programmes against hepatitis B in The Netherlands: Assessing whether a targeted or a universal approach is appropriate”. This long, convoluted self-justifying article gives an extensive review on the Hepatitis B situation in the Netherlands; what is known; what is not; and the statistical tinkering by the committee which recommended universal vaccination. This article should be compulsory reading for all thinking parents, psychology students, and epidemiologists world-wide.
Universal Hepatitis B vaccination has been recommended for all babies, primarily BECAUSE three at-risk groups are not interested in taking responsibility for their own health. Since 2003 in Netherlands, vaccination strategies have targeted three general groups:
1) Children whose mothers carry the virus;
2) Children with one parent from a country where hepatitis B is prevalent.
3) People whose behavior predisposes to hepatitis B infection. This last group included men who have sex with men, problematic drug users, commercial sex workers, and heterosexuals with a variety of sexual partners. However, molecular research showed that heterosexual contacts aren’t responsible for an infection chain of any importance, so vaccination of heterosexual men and women who "played the field", was discontinued in November 2007.
Which leaves men who have sex with men, problematic drug users, and commercial sex workers. (No mention of those who have sex with commercial sex workers!)
The article states that vaccination has largely eliminated infection in children with at least one parent from a high prevalence country, and implies that the same applies with carrier mothers.
When it come to the drug users, prostitutes and homosexuals, the article says, “In the Netherlands, a marked reduction of disease incidence has been achieved by behavioural change and targeted vaccination of specific risk groups.”
If a “marked reduction” has taken place since 2003, why vaccinate all babies?
The authors say that rates of hep B susceptibility in at risk groups are 48 – 72%; vaccination rates between 0% and 42%, and current strategies “fail to reach most people” and, “….given the already extensive efforts it seems that the potential for further improvement is limited.”.
A justification for vaccinating all babies is that you can’t work out in advance who will become a drug addict, prostitute or a homosexual.
Hepatitis virus genotyping shows that different hepatitis B virus types circulate in different groups. The hepatitis B spreading between men having sex with men, is spreading within one large sexual network. Completely different genotypes of Hepatitis B circulate in the “ordinary” community. Therefore the at risk communities do not impact on the rest of society, according to this article.
Across the whole Netherland population, acute hepatitis B infections rates are 1.4 to 2.0 per 100,000 persons.
The rate of infection in at risk groups is far far higher than that, because the data is diluted by the majority who don’t get it. Therefore the strike rate for ordinary people is lower than 1.4 per 100,000.
Every year about 200 – 300 cases of acute Hepatitis B ..and 1,500 cases and 23 deaths from chronic Hepatitis B are reported. Presumably, ... mostly in the high risk groups.
First, let’s look at Netherlands disease decline graph:
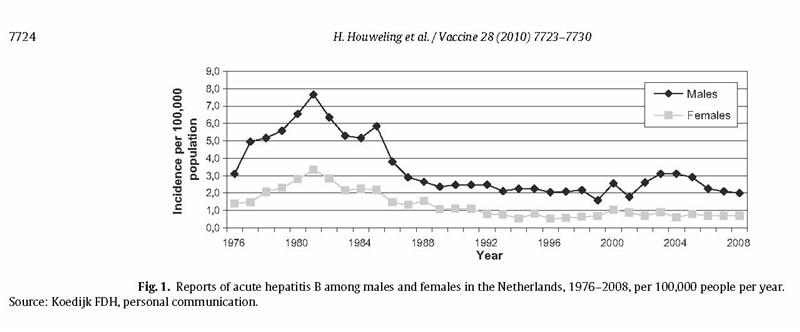
The decline above, is attributed to “changes in sexual risk behavior – whether or not in connection with the AIDS epidemic – and to preventive measures including vaccination”. On the other hand, the article bemoans the lack of vaccination and lack of progress in these at risk groups.
Which is it to be?
There has been a continued explosive increase in other sexually transmitted diseases in the Netherlands. See here, and here. This same pattern is happening everywhere in the world, where certain moral standards drives behavior. See here and here.
To suggest that safe sex reduces Hepatitis B, yet continues to allowed an explosion of other sexually transmitted diseases, is an oxymoron.
So what really caused the reduction in Hepatitis B in the Netherlands?
What follows is an educated guess:
In 1973 I got glandular fever. Every week, the laboratory would send a lab nurse to our house to take blood samples. At the same time the nurse would collect blood from my doctor’s son, who also had Glandular Fever along with many other people. The lab nurses were fantastic, even though we jokingly called them “the vampires”. In those days, there was no laboratory test to detect that specific type of hepatitis, so they called Hepatitis B, “serum hepatitis”. Everything in the laboratory was sterilized and needles autoclaved. A batch of needles was contaminated, and so all of us on that round, got hepatitis B at the same time. For many years, many people who got blood transfusions were also contaminated with Hepatitis B, becuase there was no test to detect it in donated blood. A similar situation existed later, with Hepatitis C.
So for many years, hepatitis B was secondarily spread within the medical system in most westernized countries in the same years as that graph shows above, through blood transfusions, laboratory tests and other medical practices. Once a test was readily available which defined Hepatitis B; transfusion blood was screened; and "once-use" needles and vacuum tubes for blood collection were used, Hepatitis B rates dropped.
In developing countries, hepatitis B was also spread by the Expanded programme of Immunisation, and continues to be spread today, through the deliberate, continued of use of reusable syringes.
The indigenous people of Alaska had never experienced hepatitis B at all until decades ago, when Inuit men in the military were vaccinated with contaminated Yellow Fever vaccine, and took hepatitis b back to their people. Within 30 years, hepatitis B had become a problem in Alaskan Inuits.
Therefore to suggest that the dropping Hepatitis B rates in Netherland resulted from changes in sexual behaviour or vaccination in a group in which they are making little progress, and therefore they want to vaccinate all babies, stretches credulity.
In 2001, the Netherlands committee concluded that insufficient data were available to assess the Hepatitis B infection risk in the population at large, and the effectiveness of a universal hepatitis B vaccination programme therefore couldn’t be assessed.
The article stated that epidemiological data to provide an accurate risk/benefit for Netherlands did not exist, and that “existing epidemiological models were not deemed suitable”.
The committee therefore used, "a mathematical model and cost-utility analysis” to provide data which does not exist.
This is what I call the crystal ball method, or the rabbit out of the hat method – to construct a model to provide the desired end point. A bit like a bodyguard of lies protecting the truth.
The results of this computer generated mathematical model will now be the official data for Netherlands, because the committee stated that these model-data “accurately represents the nature of HBV infection and it’s spread in the population”.
If they know this data is accurate … why did they have to make it up in the first place?
On the basis of these computer generated figures, the committee recommended that universal vaccination be implemented in three ways at the same time:
- Three shots to infants (three half shots concurrent with other vaccinations); and
- Five shots to pre-adolescents (three half shots and two full doses later) would, over 50 years, prevent 5000 deaths. The committee also suggested
- A catch-up campaign of all children, because over 50 years that would prevent an additional 650 deaths amongst some of those people who would later go on to be part of the drug users, homosexual and prostitute groups.
The committee also considered recommending vaccinating girls along with the HPV vaccine, but decided this wasn’t practical because of, “”untoward discussion in the lay and scientific media has resulted in so far insufficient uptake of that vaccination.” Other articles show the HPV uptake to be about 38%.
The Minister of Health implemented universal Hepatitis B vaccination on all babies, with another vaccine which has the Hepatitis B vaccination included in it, removing the need for another injection.
Suggestions 2 and 3 were rejected.
Compliance is expected to be high for the new baby vaccine presumably because most parents won’t ask questions because they will see the same number of needles as before.
The experts stated that because Hepatitis B vaccine is marvellously safe, and cannot cause Multiple Sclerosis or anything else bad, the risk benefit analysis is wonderful.
The existing targeted programmes to at risk groups will be continued until all groups are “protected” by neonatal universal vaccination.
So :
All Dutch families in whom hepatitis B has been no big deal in the past, will now be expected to vaccinate their babies with the hepatitis B vaccine because three at risk groups continue to be disinterested in taking responsibility for their own health.
In my opinion, the real reason is to find a way to comply with the WHO mandate that everyone, everywhere must be vaccinated with the Hepatitis B vaccine as soon as possible.
And to do that, ... they had to construct data which did not exist before, and write a long convoluted study to justify that.
There was no declaration of conflicts of interest from anyone authoring this study, or in this group of people mentioned at the end of the article:
The NIP Review Committee consists of the following persons
(all members with a right to vote unless stated ‘advisor’):
E.J. Ruitenberg, PhD, Prof. of International Public Health, VU
University, Amsterdam, Chairman; J.J. Roord, MD, PhD, Prof. of
Paediatrics, VU University, Amsterdam, Vice Chairman; M.A.E.
Conyn-van Spaendonck, MD, PhD, epidemiologist, NIP Manager,
National Institute for Public Health and the Environment (RIVM),
Bilthoven, advisor; P.J. van Dalen, PhD, Ministry of Health, Welfare
and Sport, The Hague, advisor; W. van Eden, MD, PhD, microbiologist,
Prof. of Veterinary Immunology, Utrecht University;
R. de Groot, MD, PhD, Prof. of Paediatrics, Radboud University
Nijmegen; H.E. de Melker, PhD, epidemiologist, RIVM, Bilthoven,
advisor; T.G.W.M. Paulussen, PhD, Sector Head Health Promotion,
TNO Quality of Life, Leiden; M.J. Postma, PhD, Prof. of
Health Economics, University of Groningen; H.C. Rümke, MD,
PhD, paediatrician and epidemiologist, University Vaccine Centre,
Rotterdam/Nijmegen; J.L. Severens, PhD, Prof. of Evaluation
in Health Care, Erasmus University Rotterdam; B.H. Stricker, PhD,
Prof. of Pharmaco-epidemiology, Erasmus University Rotterdam;
S.P. Verloove-Vanhorick, MD, PhD, Em. Prof. of Child Health, Leiden
University, Leiden; H.J. Vermeulen-Schakel, MD, health centre
physician, Municipal Health Service Kennemerland, Hoofddorp; M.
Verweij, PhD, ethicist, Utrecht University; A.C.G. Voordouw, MD,
MPH, PhD, Medicines Evaluation Board (CBG), The Hague, advisor;
H.L. Zaaijer, MD, PhD, Prof. of Microbiology, Academic Medical
Center (AMC), Amsterdam; H. Houweling, MD, PhD, epidemiologist,
Health Council, The Hague, Senior Scientific Officer; C.F.W.
Wittevrongel MSc, Health Council, The Hague, Scientific Officer
(until 1 January 2010).